Abstract
This paper seeks to review whether the ketogenic and low carbohydrate diets can offer cognitive protection in a wide array of cognitive impairments in both rodent and human models compared to non-ketogenic/ low carbohydrate diets. Alzheimer’s disease and dementia are used as age-related sources of cognitive decline. While diseases related to insulin resistance, inborn errors of metabolism, and epilepsy are addressed as non-aged related sources of mental decline. There is evidence to support the neuroprotective nature of carbohydrate resisted diets. However, the beneficial effects on cognition are more pronounced in individuals with pre-existing hypometabolism in the brain, related to an inability to use glucose as energy within the brain.
- Introduction
Cognitive decline happens for several reasons throughout the lifespan. For example, it is expected with age, but some people do not experience the same level of decline as others. What makes them different or rather how can that be mimicked in brains that do, unfortunately, decline faster than others? A case report examined 3 patients with mild behavioral impairment, which is a marker of cognitive decline related to age. All of these patients had significant brain atrophy related to hypometabolism of the brain.1 This happens when the brain cannot use carbohydrates for energy anymore, or as effectively.2
Hernandez et al., has found compelling research linking a decline in the ability to utilize glucose in specific parts of the brain with age, hippocampus (HPC) and prefrontal cortex (PFC). If we can supplement the brain with ketones, bypassing the need for glucose he hypothesized better interaction between HPC and PFC, as communication between these two parts of the brain tends to lessen with age and glucose utilization. They test these findings themselves using 4-month-old rats: 16 male & 2 female. There was also a grouping of 20-month-old rats 18 male and 3 female. Some rats were placed on a KD while others were put on a placebo/ control diet (CD) (of equal number). Weeks 1-22 found KD had a significant effect on b-hydroxybutyrate levels (BHB) with a statistically significant decline in glucose to inversely mirror BHB. While the controls continue to increase their blood glucose and maintain steady levels in BHB. To test the effect of the KD on cognition a series of tests were performed by the rats, such as an elevated figure 8-shaped maze with two arms containing food. The KD rats were found to learn the maze faster than the control (p= 0.01). They also showed greater resilience in their ability to overcome anxiety. By spending significantly less time in the closed arms than controls, especially on day 20 when the KD group were the first ones to meet the criteria for performance. It should be noted that on day 12, the KD rats reached ≥ 80% criteria for performance. The next test was a working memory/bi-conditional task (WM/BAT), this tests the communication between PFC-HPC. There was a small period, day 12 -15, where statistically significant results showed an increase in performance on the WM/BAT in KD vs control, p < 0.05 and age p = 0.03. The random arm bi-conditional association task (BAT) was employed to avoid spatial reasoning bias among subjects, was not found to statistically significant. This data is in line with findings from Ota et. al. (2016), which suggested higher ketone levels may alleviate the negative side effects of declining glucose metabolism in the elderly, as an alternative fuel source for the brain.3 Day 13 presented with a potential source of bias due to technical issues. The researchers needed to retest 6 young mice and 7 aged ones. They provide that it happened to both the KD and CD equally. However, they did not provide a count of the rat’s sex in each group. They claim that the influence was similar to both groups but fail to provide statistical data or evidence of such.4
There are also those who have cognitive impairment related to reasons other than age. Age may actually be exacerbated by impaired insulin functioning, which can result in physical manifestations of obesity, metabolic syndrome, type two diabetes mellitus, etc. Those with altered insulin resistance do not only suffer from the physical side effects but are also at much higher odds of developing Alzheimer’s disease or dementia.5
Iacovides et al., studied the effect of the ketogenic diet (KD) on cognition and sleep (which affects general mental power) over a 3-week window in healthy, non-obese men (n=1) and women (n=10) 30 years plus or minus 9 years. They compared an isocaloric KD and high carb low fat (HCLF) diet. Participants were asked to log their food on MyFitnessPal, where the data could be evaluated over the course of the study. Each participant followed the assigned diet for three weeks, had one washout week and then moved over the alternative diet. It was designed as a randomized, controlled, crossover trial. The researchers made sure each participant was in nutritional ketosis (> 0.4 mmol/L of b-hydroxybutyrate (BHB) blood tests). A series of questionnaires were the mode of testing for cognition and sleep/ mood assessments. The Cogstate psychological test was used as an assessment for cognitive ability. The subjects were asked to fill out The Pittsburgh Sleep Quality Index (PSQI) and a 100-mm visual analog scale of their sleep quality and mood once before bed and once upon waking, respectively. After 3 weeks the study had no statistically significant findings on the effect of the ketogenic diet on the improvement of cognition or sleep quality. However, marginal findings were found in the HCLF for improved processing speed first thing in the morning. KD was found to slightly improve processing speeds in executive function and working memory compared to the HCLF diet. One confounding variable was the small sample size of n =11 participants. Of which, one was male and no comment on the women’s cycle was accounted for (or if she was menstruating at all/ entered into menopause).6
Newman et al., finds the KD can preserve memory in male mice into old age (2.5 years). The aim was to get plasma beta-hydroxybutyrate (BHB) levels as high possible, without comprising health in order to study the benefits of KD induced BHB on health. Five diets total were tested. The control diet was standard AIN-93M, altering in lipid and CHO content, but equivalent kcal to other diets, vitamins, minerals, fiber, and protein. The other diets were: zero CHO KD, HF (high fat) non-keto diet, cyclic (every other week) KD/ AIN-93M, cyclic (every other week) HF/ AIN-93M. BHB levels were higher on KD cyclic vs plain KD mice. Memory was improved with aged mice on the KD. The mechanism responsible is believed to be BHB. This study differentiated mechanism of KD and LCHF. While they have many similar pathways, peroxisome proliferator-activated receptor alpha (PPAR-a) signaling is distinctive to the KD. Dr. Newman mentions that deacetylase inhibition may be linked to the preservation of memory, induced by BHB modulation. This study contrasts Brownlow et al. (2013) by demonstrating that their mice showed no motor improvement with the KD. However, differences in age and species may confound this comparison. Potential sources of bias in this comprehensive study include sex, the study only looked at male mice. It should be noted that the strain used for this study is known for longevity independent of the ketogenic or low carb high-fat diets.7
The purpose of this review is to determine whether the ketogenic and low carbohydrate diets can offer cognitive protection in a wide array of cognitive impairments in both rodent and human models compared to non-ketogenic/ low carbohydrate diets.
Age related decline
Brownlow et al., studied underlying pathologies of amyloid-beta (ab) deposition and tau deposition were differentiated relating to the KD (ketogenic diet). On the basis that KD provides alternative fuel sources for the brain and can potentially bypass the negative effects of each. They wanted to see if each pathway had a different benefit by isolating the two neurofibrillary tangles of Alzheimer’s and dementia. To do this they studied 3 populations of 5 month old mice non-transgenic controls (n=10 KD and n= 10 standard/ NIH-31), transgenic APP+PS1 (amyloid precursor) (n=10 KD and n= 10 standard/ NIH-31), and transgenic Tg4510 (tau depositing mice) (n=10 KD and n= 10 standard/ NIH-31) over a 3 month window. The mice were either given KD or a standard diet (NIH-31). The open field test, walled Y-maze, radial arm water maze (RAWM), and fear conditioning were used as cognitive testing. The researchers found that there was a greater effect in BHB levels in the nontransgenic mice compared to transgenic mice (APP+PS1and Tg4510) p<0.0001, showing a significant genotype interlinkage p = 0.021. Another interesting find was that glucose levels were persistently lower in all KD fed subjects, but lower in nontransgenic mice compared to both APP+PS1 and Tg4510. This relationship had a p-value of 0.0001. BHB was highest in blood samples in week 16 (3.6 months). Nontransgenic mice also ate more than the other two populations, yet has a smaller BMI (p<0.0001). This is interesting as a lower BMI is linked to being neuroprotective.8 Both transgenic mice explored the furthest in the open field test compared to nontransgenic mice (p<0.0001). Interestingly, the Tg4510 mice the most activity, even compared to the APP+PSI stain (p=0.002). They also had a statistically significant amount of Y-maze arm entries and a higher percentage of alteration in arms (p=0.02). Brownlow et al. suggested this may be due to a hyperactive phenotype. Despite the mice showing no improvement in memory deficits, the KD mice (across all populations) did improve their motor activity (p<0.007). There was no neural protection offered by the KD in any population nor changes in overturning tau or amyloid-beta. There did not seem to be any neuroprotective mechanisms observed with the KD in this study. This study fits with Paoli et al. (2012) in the relationship of KD sparing lean mass in favor of muscle and having an increased benefit on physical activity. A possible confound was not testing blood ketone and glucose levels frequently enough, ideally this should be done the same week that behavioral testing was administered. The result of this paper indicates that the KD does not seem to improve cognition. Although, subjects were induced with a genetic predisposition to Ab and Tau deposits in the brain.9
Ota et al., studied the effect of MCTs (medium-chain triglycerides) on the enhancement of mental functions in the non-demented elderly Japanese population. Contrary to a recent study by Ota et al. (2019), that did not find short-term significant improvements on cognition in patients with Alzheimer’s disease (AD), their 2016 study did. Noted in baseline groups where b-hydroxybutyrate (a ketone) was much lower in baseline measurements. This suggests that MCTs may be even more effective in people with already impaired glucose metabolism. Another interesting finding was that some patients seemed to display higher b-hydroxybutyrate levels at 90 min postprandial, while others had higher b-hydroxybutyrate levels at 180 minutes compared to placebos. Cognitive test scores were statistically higher in subjects with increased b-hydroxybutyrate with a correlation coefficient = 0.49. Ota et al. (2016) even studied MCT content of previous studies to consist of 95% caprylic acid. They modeled their meals with 15 g caprylic acid and 5 g capric acid, there is evidence to support increased astrocyte ketogenesis in caprylic acid vs capric acid. Unlike Ota et al. 2019, they found other studies to support acute efficacy of cognitive performance in patients with AD. It is thought that ketones can act as an alternative fuel to CHO (carbohydrates). Ota et al. have found that a negative relationship exists in glucose metabolism of the aging brain. This leads to the proposed idea that MCTs could fuel the aging brain with ketones to counteract the effects of impaired glucose metabolism. It is worth noting that the only significant effects of the KD were in patients with lower baseline cognitive test scores than higher scoring individuals. Suggesting that this beneficial effect may only be seen in people with impaired glucose regulation (perhaps a level of decline in cognition as well). This study was also restricted in its sample size at 20 adults > 60 years old. They made special efforts to avoid practice effect by changing the order in which meals were provided. Overall this article shows promising evidence that 20 g MCTs (15 g caprylic acid, 5 g capric acid) does increase blood ketone levels 90 -180 minutes out, with statistically significant improvements in working memory and executive function. This is a novel study, due to its use of patients without dementia or AD.3
A study conducted by Ota et al. (2019), over a 12 week period on 20 patients (n= 11 male, n=9 female, aged 73.4 ± 6 years) with Alzheimer’s Disease (AD) tested the effects of the KD on intellectual operations. There were no statistically significant findings on immediate postprandial consumption of the ketogenic formula, which was based on medium chain triglycerides (MCTs). However, longer term consumption (2-3 months) showed significant improvement in working memory, processing speed, and short-term recall as shown in figure 2. Wechsler Memory Scale- Revised (WMS-R) cognitive test measures immediate and delayed memory, along with digit and visual memory span. A higher score on the WMS-R indicates increased cognitive functioning (a p value less than 0.05 is considered statistically significant). Logical and delayed memory were statistically significant, as reflected by p = 0.001 for immediate and p = 0.005 for delayed memory. Similar findings were present in an earlier study conducted by Ota et al. In 2016, WMS-R (and Trail Making Test, measure of attention span: visual attention and task switching) values were statistically significant at 90 and 180 minutes: p= 0.024 and p= 0.045 respectively. Increased blood levels of BHB in the patients was associated with increased cognitive test score p= 0.042), indicating improved cognition in working memory (and attention).3 A few limitations of the Ota et al. (2016) study, was the small sample size (n=20) and population diversity only varied in sex of the patients who were otherwise homogenous elderly Japanese citizens with neurodegenerative disorders. Note that there were no non-diseased controls.10
Non-age-related decline
Findings from Dr. Gyorkos et al. indicate that a carbohydrate restricted, Paleolithic-based diet (CRPD) with exercise increases brain-derived neurotrophic factor (BDNF) in patients with metabolic syndrome (MetS). BDNF plays a key role in neuroplasticity and overall cognitive functioning. There were 12 participants total, both men (n=4) and women (n=8) with MetS enrolled in this study (an obvious limitation) from there they were randomized into LC sedentary (CRPD-sed, n=5) group and a low carb exercise (CRPD-ex, n =7) group (no control was used, another limitation of the study). Exercise is known to increase levels of ketones in the body, especially BHB.2 Phase 1 lasted 4 weeks, then a washout period of 4 weeks took place for both groups before crossing over to the opposite diet and exercise regimen for an additional 4 weeks. Carbs were resisted to < 50 g/d with unlimited access to protein and non-starchy veggies, while moderated amount of nuts, potatoes, and wine were allowed and no dairy, grains, beans, or other high processed/ carbohydrate containing foods were allowed. Subjects exercised 3 days/ wk for 4 weeks with high intensity interval training (HITT). The Stroop test was used to gauge speed and flexibility in cognition, the lower the number indicates a quicker/ more favorable test time. Figure 1 indicates statistically improved cognitive functioning for each group (p < 0.05), notably the exercise group had the largest improvement from baseline in cognitive flexibility 5.9 ± 1.2 to post 4 weeks 3.2 ± 0.6.11
Benjamin et al., wanted to test if the KD would be beneficial to patients with Kabuki Syndrome (KS). KS is defined as a genetic mutation that has faulty neuronal functioning, impairing physical growth, low cognitive performance, distinct facial features and immunity dysregulation. Normal drug intervention would call for the use of histone deacetylase inhibitors (HDACis) in the form of HDACi AR-42. However, this does not come without potentially lethal side effects. This brings forth an alternative route to recovery. The researchers have found supporting evidence that beta-hydroxybutyrate (BHB) has HDACis activity, but without the side effects of the medication.12
When BHB is flowing freely throughout the body it is continuously being transferred into the CNS where it can directly enter the hippocampus. Which would make it readily available to histone alterations in neurons. The expected outcome would be to improve neurogenesis in these individuals with KS. Benjamin was able to isolate BHB from the KD, effects via exogenous BHB. They continued to increase BHB supplementation until the benefits matched that of the KD. This study supports that the KD integrated the phosphorylated histone modification, improving neurogenesis and memory. The main mechanism of action here was speculated to be related to cellular NADH/ NAD+ ratio reflective of BHB to AA (acetoacetate). ATP production was controlled for. This article supports other claims that BHB is the main therapeutic effect of the KD and generalized neuronal protection (Newman et al. 2017).7,13 Potential sources of bias: small sample size (a common theme of these studies) and a short testing duration, as noted by Hernandez et al. (2018), we tend to see a peak in performance mid KD initiation.12
Noh et al. discovered beneficial mechanisms behind the KD (ketogenic diet) when used to treat epileptic patients. Epilepsy can harm cognitive function. This effect can cause similar accumulation of amyloid-beta and tau as seen in AD patients, figure 3, research conducted by Gourmaud et al.14 Neuronal excitability has been noted by increased levels of Ca2+, related to seizures. KD causes calcium-binding protein calbindin to protect the brain by cleaning up excessive Ca2+. Seizures seem to have a relationship with proapoptotic proteins in the hippocampus. One of which (nuclear clusterin) did not accumulate with KD. Triggers for limbic related seizures are related to more proapoptotic proteins, such as Bad, Bax, and caspase-3. When fed KD an increase in antiapoptotic factors was seen such as, Akt-p, 14-3-3, and Bcl-xL. The research team found that the KD has serval neuroprotective operations related to inhibition ROS (reactive oxidative species) and PENK gene pathway.A precursor to ROS damage is glutamate activation, when ketones acetoacetate (AA) and beta-hydroxybutyrate (BHB) were put into the hippocampal lining of murine brains (HT22) it decreased ROS levels overall. Noh et al., discovered that HT22 was protected due to glutamate toxicity. With glutamate destroyed the production of ROS went down within the hippocampal lining. Opioid peptides and glutamate synchronize with each other. One of these opioid peptides is extracted from proenkephalin (PENK). Noh, established that the levels of PENK were significantly decreased in the dentate granule cells (of the hippocampus) in KD treated subjects. These findings are supported by Hallbook et al. (2012), in the improvement of mitochondrial functioning related to decreased production of ROS due to the KD. Noh et al. shows a benefit of KD on the hippocampal preservation.15
- Conclusions
The ketogenic diet shows therapeutic promise in patients with cognitive decline, regardless of origin. The majority of the studies reviewed support that the ketogenic diet has neuroprotective mechanisms and/or considered non-harmful.5 There is either a positive effect or no effect. None of these articles suggest that there are negative side effects of the ketogenic diet when malnutrition is avoided. Although, the neuroprotective effects seem to be more pronounced in individuals who already have issues utilizing glucose in the brain (or hypometabolism).
Hallbook et at. 2012 wrote a review on the KD role in epilepsy, sleep, and cognition via experimental and clinical findings. This study emphasizes the need for standardization among KD experiments, as the potential for this to be a primary therapy for not only epilepsy, but other potential neurological disorders and others related to glucose metabolism may prove to be worth the extra data of future experiments.
The KD was associated with impaired brain growth resulting in gaps related to memory and spatial learning. However, Cunnane and Likhodii (2004) explain that these ill side effects could be a result of poor nutrition related to improper administration of the KD. The KD is safe when properly administered.
Hallbook et al., also notes that REM (rapid eye movement) and SWS (slow wave sleep) are both affected by the KD. In patients with epilepsy after treatment with KD show decreased time of sleep, but increased sleep quality by more REM sleep then SWS. SWS has been the most provocative of seizure induced activity. With increased REM there was also noted daytime alertness in patients receiving the KD vs ones who were not and fewer naps during the day. The different types of sleeping patterns may be regulated by the KD and can affect the KD has to potential to be in regulating them. Sleep quality is support for Noh et al., regarding ROS and anti-apoptotic activity, which play a role circadian rhythms regulation.16
Astrup and Hjorth, explored if people with type two diabetes mellitus (T2DM) could improve their quality of life with the KD. In this review they translate animal models into potential benefits for humans. Although, they make sure to point out physiological differences. For instance, mice are prone to developing obesity and generalized adiposity with KD and low carb (LC) diets. Whereas human models of these diets do not have the same outcomes. The KD was beneficial in decreasing cognitive decline related to age, and a lower risk of midlife death. This paper is in line with many other sources, supporting the differentiation of KD and LC.7 That the KD shows much more benefits than LC. This article has helped put the KD in perspective of rodent studies vs human implementation and the differences we need to consider in metabolism.17 However, more studies should be conducted to isolate if the benefit is from the ketogenic itself or the challenge/ stress that is placed on metabolic systems after we have worn out one metabolic pathway versus another.
References
1. Cieslak A, Smith EE, Lysack J, Ismail Z. Case series of mild behavioral impairment: toward an understanding of the early stages of neurodegenerative diseases affecting behavior and cognition. International Psychogeriatrics. 2018;30(2):273-280. doi:10.1017/S1041610217001855
2. Camandola S, Mattson MP. Brain metabolism in health, aging, and neurodegeneration. The EMBO Journal. 2017;36(11):1474-1492. doi:10.15252/embj.201695810
3. Ota M, Matsuo J, Ishida I, et al. Effect of a ketogenic meal on cognitive function in elderly adults: potential for cognitive enhancement. Psychopharmacology. 2016;233(21-22):3797-3802. doi:10.1007/s00213-016-4414-7
4. Hernandez AR, Hernandez CM, Campos K, et al. A Ketogenic Diet Improves Cognition and Has Biochemical Effects in Prefrontal Cortex That Are Dissociable From Hippocampus. Frontiers in Aging Neuroscience. 2018;10:391. doi:10.3389/FNAGI.2018.00391
5. Murray AJ, Knight NS, Cole MA, et al. Novel ketone diet enhances physical and cognitive performance. FASEB journal : official publication of the Federation of American Societies for Experimental Biology. 2016;30(12):4021-4032. doi:10.1096/fj.201600773R
6. Iacovides S, Goble D, Paterson B, Meiring RM. Three consecutive weeks of nutritional ketosis has no effect on cognitive function, sleep, and mood compared with a high-carbohydrate, low-fat diet in healthy individuals: a randomized, crossover, controlled trial. The American Journal of Clinical Nutrition. 2019;110(2):349-357. doi:10.1093/ajcn/nqz073
7. Newman JC, Covarrubias AJ, Zhao M, et al. Ketogenic Diet Reduces Midlife Mortality and Improves Memory in Aging Mice. Cell metabolism. 2017;26(3):547-557.e8. doi:10.1016/j.cmet.2017.08.004
8. Schmoller A, Hass T, Strugovshchikova O, et al. Evidence for a relationship between body mass and energy metabolism in the human brain. Journal of cerebral blood flow and metabolism : official journal of the International Society of Cerebral Blood Flow and Metabolism. 2010;30(7):1403-1410. doi:10.1038/jcbfm.2010.48
9. Brownlow ML, Benner L, D’Agostino D, Gordon MN, Morgan D. Ketogenic diet improves motor performance but not cognition in two mouse models of Alzheimer’s pathology. PloS one. 2013;8(9):e75713. doi:10.1371/journal.pone.0075713
10. Ota M, Matsuo J, Ishida I, et al. Effects of a medium-chain triglyceride-based ketogenic formula on cognitive function in patients with mild-to-moderate Alzheimer’s disease. Neuroscience Letters. 2019;690:232-236. doi:10.1016/J.NEULET.2018.10.048
11. Gyorkos A, Baker MH, Miutz LN, Lown DA, Jones MA, Houghton-Rahrig LD. Carbohydrate-restricted Diet and Exercise Increase Brain-derived Neurotrophic Factor and Cognitive Function: A Randomized Crossover Trial. Cureus. 2019;11(9):e5604. doi:10.7759/cureus.5604
12. Benjamin JS, Pilarowski GO, Carosso GA, et al. A ketogenic diet rescues hippocampal memory defects in a mouse model of Kabuki syndrome. Proceedings of the National Academy of Sciences of the United States of America. 2017;114(1):125-130. doi:10.1073/pnas.1611431114
13. Newman JC, Verdin E. β-Hydroxybutyrate: A Signaling Metabolite. Annual review of nutrition. 2017;37:51-76. doi:10.1146/annurev-nutr-071816-064916
14. Gourmaud S, Shou H, Irwin DJ, et al. Alzheimer-like amyloid and tau alterations associated with cognitive deficit in temporal lobe epilepsy. Brain. December 2019. doi:10.1093/brain/awz381
15. Noh HS, Kim YS, Choi WS. Neuroprotective effects of the ketogenic diet. In: Epilepsia. Vol 49. ; 2008:120-123. doi:10.1111/j.1528-1167.2008.01855.x
16. Hallböök T, Ji S, Maudsley S, Martin B. The effects of the ketogenic diet on behavior and cognition. Epilepsy research. 2012;100(3):304-309. doi:10.1016/j.eplepsyres.2011.04.017
17. Astrup A, Hjorth MF. Improvement in age-related cognitive functions and life expectancy by ketogenic diets. Nature Reviews Endocrinology. 2017;13(12):695-696. doi:10.1038/nrendo.2017.142
Abbreviations
AA – acetoacetate
AD – Alzheimer’s disease
BDNF – brain derived neurotropic factor
BHB – beta-hydroxybutyrate
CCK – cholecystokinin
CD – control diet
CHO – carbohydrates
HDACis – histone deacetylase inhibitors
HT22 – hippocampal lining of murine brains
KS – Kabuki Syndrome
KD – Ketogenic diet
LC – low carbohydrate
MetS – metabolic syndrome
MCT – medium chain triglyceride
PENK – proenkephalin
PPAR-a – Peroxisome proliferator-activated receptor alpha
PSQI – Pittsburgh Sleep Quality Index
REM – rapid eye movement
ROS – reactive oxidative species
T2DM – type two diabetes mellitus
SWS – slow wave sleep
Supplementary Material
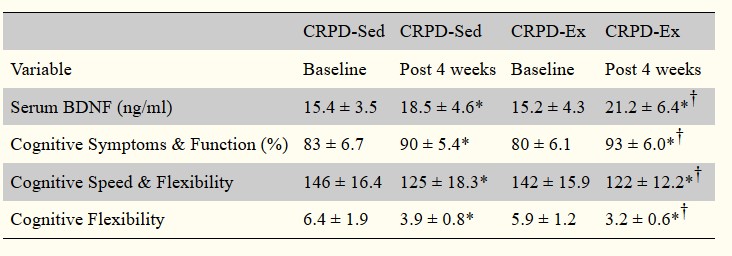
Figure 1. Gyorkos et al. 2019 An increase in BDNF leads to neuroplasticity. The Stroop test was used as a measure of cognitive functioning, the lower the score the faster the test was performed. The data here shows improved cognitive functioning with the carbohydrate restricted diet.
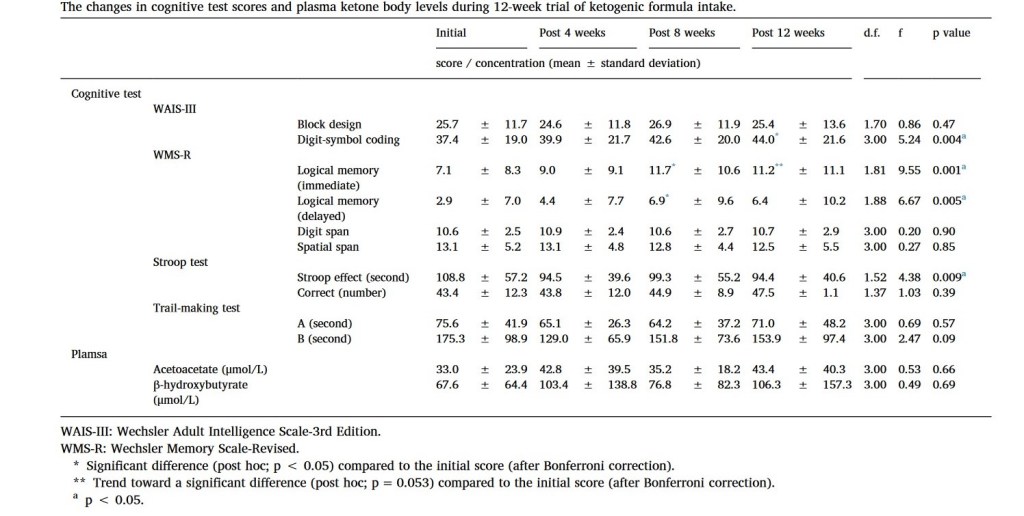
Figure 2. Ota et al. 2019 A p value less than 0.05 is statistically significant. Logical memory immediate and delayed show significant improvements on the WMS-R cognitive test with the ketogenic diet over 12 weeks.
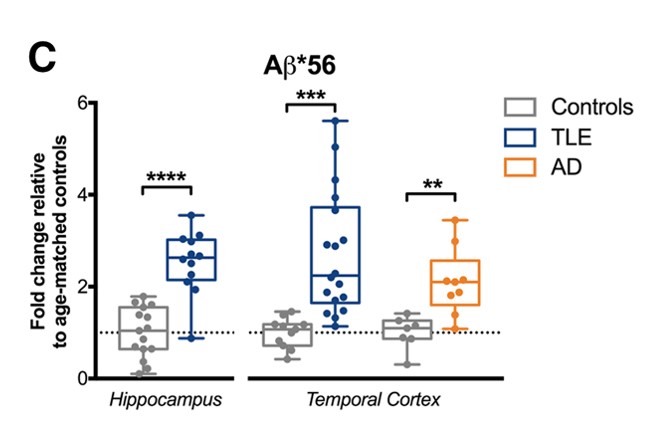
Figure 3. Gourmaud et al. 2019 TLE – Temporal Cortex Epilepsy, AD- Alzheimer’s Disease. Statistical significance is indicated by the asterisk. The more asterisk the greater the statistical significance.



Leave a comment